It was an old known case of heart attack. The gentleman was 55 years old. Recently he started developing pedal edema, that is swollen feet.
Apparently, all else was ok.
The patient had undergone FDG PET nuclear imaging scan for his condition and also echocardiography. He was diagnosed with apical and septal myocardial ischaemia. That was 7 years ago and since then he was on treatment.
Now had he reported to his family clinician for his current condition.
The physician advised for fresh echocardiography to look into condition of the heart. The patient arrived at ARDISS IMAGING AND DIAGNOSTIC CENTRE for the same.
On scanning, the right ventricle and atrium were dilated. The IVC was also dilated with reduced inspiratory collapsibility. The Left ventricle showed mild reduced pumping capacity with regional wall motion abnormality in the apical and septal region.
The flow rates were higher at tricuspid valve and pulmonary artery compared to the bicuspid valve and aorta.
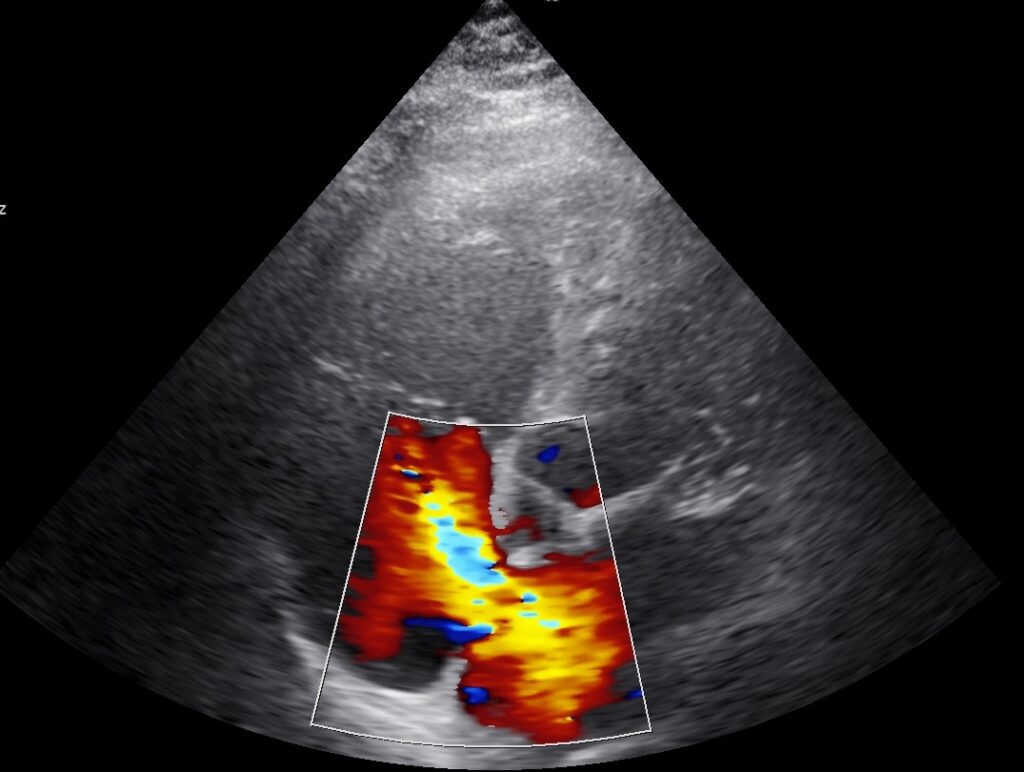
Hemodynamically, things were not explainable. A second look into colour images was taken. And, there it was, a defect in the wall separating the two upper chambers, the atria. Flow was noted from Left to Right atria through this 9 mm sized atrial septal defect, giving the right sided chambers extra amount of blood to handle. That caused the dilatation of the right atrium, right ventricle and IVC. That also caused high flow through lungs resulting in raised pulmonary arterial pressure.
All this led to the oozing of fluid, causing the pedal edema. Thus, the mystery was solved.
